Shocking State Secrets: How 1 in 5 Medicaid Enrollees Are Denied Crucial Contraceptive Care!
Medicaid serves as a crucial safety net for millions of low-income individuals seeking access to contraceptive care across the United States. In fact, it is the largest publicly funded program financing family planning services, enabling a network of providers, including Planned Parenthood clinics, community health centers, state and local health departments, and Indian Health Services, to deliver essential reproductive health services. However, the landscape of these providers varies greatly from state to state, impacting how female Medicaid enrollees access contraceptive care.
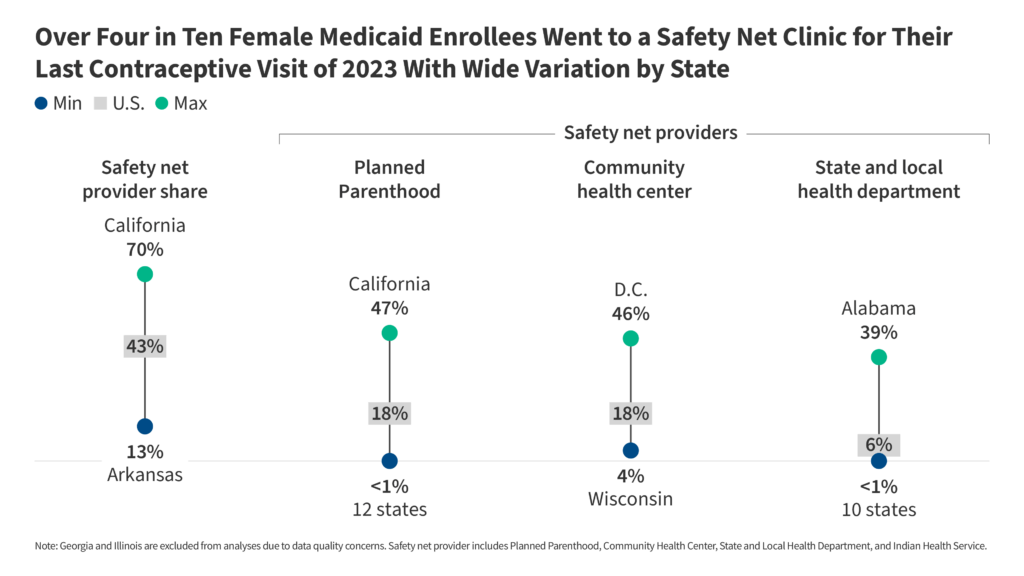
Nationally, over four in ten (43%) female Medicaid enrollees cited that their most recent contraceptive visit in 2023 occurred at a safety net provider. While this network is significant, it's important to note that a majority (54%) of female Medicaid enrollees visited office-based providers or outpatient clinics for their last contraceptive care. The reliance on safety net providers varies considerably; for instance, community health centers (CHCs) accounted for 18% of recent contraceptive visits, with rates peaking at 46% in Washington, D.C., while falling to just 4% in Wisconsin. Similarly, Planned Parenthood, another pivotal source, also represented 18% of visits but saw stark disparity across states—California reported that 47% of female Medicaid enrollees accessed care from Planned Parenthood, whereas many states, including Arkansas and Texas, reported zero visits.
Health departments and Indian Health Services played smaller roles overall, accounting for 6% and 1% of visits, respectively. However, in states like Alabama, a remarkable 39% of female Medicaid patients received their last contraceptive visit through health departments. This demonstrates the vital role that local programs can have in certain regions.
The effectiveness of the reproductive health safety net is currently under threat due to recent policy changes and funding cuts initiated by the Trump Administration. In June 2025, the Supreme Court's ruling in the case of Medina v. Planned Parenthood South Atlantic allowed states to exclude Planned Parenthood from their Medicaid programs. This was compounded in July 2025 when the Federal Budget Reconciliation Law was enacted, which temporarily prohibited federal funding for Planned Parenthood and similar family planning providers. These changes have led to significant uncertainties regarding the availability of contraceptive services, particularly as many Planned Parenthood clinics have shut down due to financial constraints.
To assess how female Medicaid enrollees accessed contraceptive care, the Kaiser Family Foundation (KFF) analyzed data from the 2023 Transformed Medicaid Statistical Information System Research Files. The study's focus was on the last location where enrollees received contraceptive care, rather than multiple visits throughout the year, thus eliminating duplicative data.
Community health centers, defined as federally qualified health centers (FQHCs) and other similar clinics, are tasked with providing a comprehensive range of health services, including contraceptive care. However, they have historically struggled to meet the demand, as previous research shows that only 25% of these centers can provide the most effective contraceptive methods on-site. Consequently, a significant increase in client volume would be required to offset the losses from Planned Parenthood closures. Overall, the national share of female Medicaid recipients who visited CHCs for contraceptive care was 18%, with substantial variation across states.
Health departments, while accounting for a smaller portion of the national landscape, have proven vital in some regions. Many state and local health departments receive Title X funding to provide family planning services. However, they have tended to serve fewer patients than Planned Parenthood and federally qualified health centers. Notably, health departments in the Southeastern U.S. have seen higher percentages of female Medicaid enrollees receiving care, with Alabama leading at 39%.
Indian Health Services provide vital care, especially in states with large Native American populations. In Alaska, for example, 37% of female Medicaid enrollees received their last contraceptive visit through IHS. However, anticipated reductions in Medicaid enrollment due to upcoming policy changes pose a risk to these crucial services.
In contrast, office-based providers and outpatient clinics remain the most common sites for contraceptive care, serving a significant majority (54%) of female Medicaid enrollees nationally. This percentage varies widely by state, presenting challenges for clinics in maintaining service levels as they face an influx of patients from closing safety net providers.
As we look ahead, the potential impacts of the 2025 Federal Budget Reconciliation Law and ongoing litigation surrounding Medicaid funding suggest a challenging future for reproductive health care access. With predictions indicating that the law could increase the uninsured population by up to 10 million over the next decade, the remaining safety net providers will likely face even greater strain.
The landscape for contraceptive care in the U.S. is shifting dramatically. With more individuals potentially facing barriers to access, it is crucial to monitor how these changes influence reproductive health outcomes, particularly among low-income populations reliant on programs like Medicaid.
You Won’t Believe What VIRTUE Asia and Goldfinch International Are Unleashing in 2023!
You Won't Believe These 5 Mind-Blowing Prop Bets for Giants vs. Patriots—One Could Make You Rich!

Bitcoin Plunges 30% Overnight! Are Investors About to Face a Total Collapse?

Kimi Antonelli's Shocking Social Media Blackout: What Red Bull's Apology Reveals About the Death Threats!

The Clock is Ticking: Are You One of the 35 Innovators Who Could Change 2026 Forever?
You Won't Believe How 7 Simple Lifestyle Changes Can Transform Your Health in Just 30 Days!
You might also like: